
Every May, the conversation turns to mental health. Hotline numbers get shared. People remind each other it’s okay not to be okay. But this Mental Health Awareness Month, a different question deserves attention: What happens when the diagnosis itself is wrong?
I have ADHD, which means I will spend an hour picking a font for a document no one else will ever see.
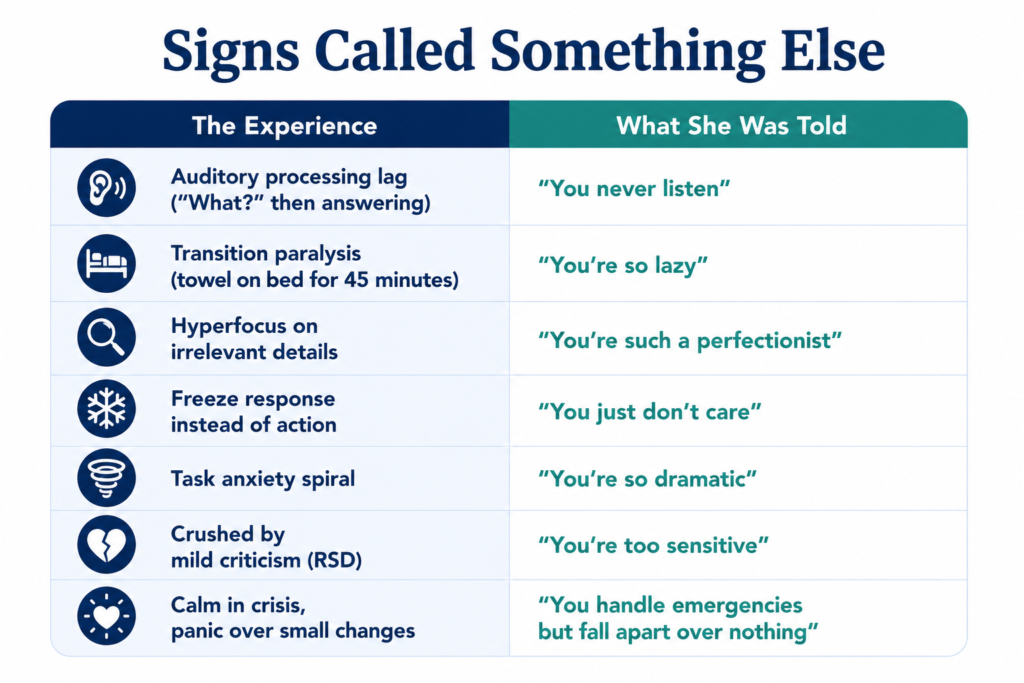
I have ADHD, which means when someone says something to me, my first response is “what?” and then I answer the question before they can repeat it.
I have ADHD, which means I sat on the edge of my bed in a towel for 45 minutes after my shower because the transition to “clothes” felt like a military operation.
I have ADHD, which means I will think about a five-minute task all day, finally do it in two minutes, and then feel inexplicable rage at myself for the next three hours.
These are not personality quirks. They are not character flaws. They are not the result of laziness, bad parenting, or a lack of discipline. They are the daily texture of a brain that works differently, a brain that, for millions of women, went undiagnosed for decades.
Nobody told these women they had ADHD. They were told they were daydreamy, too sensitive, dramatic, disorganized, bad with money, bad with time, bad at being a girl the right way.
They were handed the wrong diagnosis, the wrong medication, the wrong explanation for why they always felt like they were failing at things other people made look easy. And by the time they got the right answer, if they got it at all, the years of white-knuckling through a world that didn’t fit their brains had already done its damage.
This is the story of what happens when a diagnosis comes too late, not just the years lost but the conditions created. The depression that developed because they couldn’t understand why everything was so hard. The anxiety that calcified from decades of masking. The chronic pain that settled into bodies held tense for too long.
The cruelest irony is that the missed diagnosis didn’t just delay treatment. It made them sick.
The Missed Girl
The woman living that reality today was once a girl nobody thought to evaluate. She was never the kid bouncing off walls or blurting out answers in class. She was the quiet one in the back, staring out the window, lost in her own world. Teachers called her a daydreamer. Her parents said she was “in her head” a lot. Report cards praised her potential but noted she needed to apply herself.
She wasn’t hyper. Her brain processed information differently, in ways the diagnostic criteria weren’t built to recognize. And because those criteria were built on studies of hyperactive boys, nobody thought to look twice.
The problem started in the 1970s, when researchers first defined what is now called ADHD. The early studies drew almost exclusively from young white boys referred to clinics for disruptive behavior. The resulting diagnostic framework emphasized external symptoms: the kid who can’t sit still, who interrupts constantly, who climbs furniture and runs into traffic.
Girls with ADHD rarely look like that. They lose track of assignments, not because they don’t care but because their brains struggle to hold and organize information. Their auditory processing works on a delay. Their brains take in information on a different timeline, which can look like distraction but isn’t. They feel overwhelmed by tasks that seem simple to everyone else.
The research confirms what these women have always suspected. Women with ADHD are diagnosed an average of five years later than men, according to Psychiatric Times, even though their symptoms appear at the same age. The delay isn’t because women develop ADHD later. It’s because clinicians aren’t trained to see it in them.
The disparity widens for women of color. Black and Latina women face compounded barriers to diagnosis, navigating both the gendered blind spots in ADHD research and the racial biases embedded in mental health care. Their symptoms are more likely to be attributed to attitude, environment, or cultural factors rather than neurology.
By the time a girl reaches adolescence, she has often learned to compensate. She develops workarounds, coping mechanisms, and elaborate systems to mask her struggles. She stays up late to finish homework that took her three times longer than it should have. She rehearses conversations in her head so she doesn’t say the wrong thing. She learns to perform “normal” so convincingly that no one notices the exhaustion underneath.
The mask works, for a while. But the cost of wearing it accumulates in ways she won’t fully understand until decades later.
The disparity widens for women of color. Black and Latina women face compounded barriers to diagnosis, navigating both the gendered blind spots in ADHD research and the racial biases embedded in mental health care. (Photo source: Canva)
The Masking Years
That accumulated cost has a name. Masking is the term for the conscious and unconscious strategies neurodivergent people use to appear “normal,” and for women with undiagnosed ADHD, masking isn’t a choice. It’s survival. And survival exacts a price.
In her teens and twenties, the undiagnosed woman builds an elaborate internal scaffolding to hold her life together. She creates systems within systems: color-coded calendars, obsessive list-making, phone alarms for everything from taking medication to remembering to eat. She over-prepares for meetings and social events, rehearsing what she’ll say so she doesn’t ramble or interrupt or forget halfway through a sentence what point she was making.
She becomes hypervigilant about other people’s reactions, scanning faces for signs of annoyance or disappointment. She apologizes constantly, preemptively, for things she hasn’t done wrong. She says yes to everything because saying no feels dangerous, like one rejection could unravel the carefully constructed image of competence she’s built.
This is often when anxiety and depression first take root, not as separate conditions but as the natural consequence of running a brain at 150% capacity just to function at baseline. The chronic stress of masking triggers the body’s fight-or-flight response, flooding the system with cortisol and adrenaline. Over time, the nervous system forgets how to return to rest.
A 2025 study in Scientific Reports found that women who received late ADHD diagnoses reported pervasive feelings of guilt, shame, and low self-esteem that had accumulated over years of struggling without explanation. Many described the eventual diagnosis as “revelatory,” a word that captures both the relief of finally understanding and the grief of realizing how much suffering could have been avoided.
The masking years are also when many women first encounter the mental health system, but they walk in with the wrong presenting complaint. They tell their doctors they’re anxious, they’re depressed, they can’t sleep, they can’t stop worrying. They’re given selective serotonin reuptake inhibitors, benzodiazepines, sleep aids, and therapy focused on cognitive distortions. All of these interventions may help manage symptoms, but none of them address the underlying cause.
Meanwhile, the undiagnosed ADHD continues to drive the bus.
The Brain at War With Itself
For some women, the diagnostic picture is even more complicated because they don’t just have ADHD. They also have autism. And the two conditions, when they occur together, create a neurological experience so contradictory it can feel like being two different people trapped in the same brain.
The term “AuDHD” has emerged in neurodivergent communities to describe this co-occurrence, though it remains a residual category rather than a formal diagnosis. Emma Craddock, a senior lecturer in health research at Birmingham City University, noted that people with both conditions often struggle to find recognition within existing diagnostic frameworks, which were designed to identify each condition in isolation.
The contradictions are relentless. The autistic brain craves routine, predictability, and sensory calm. The ADHD brain craves novelty, spontaneity, and stimulation. The result is a person who desperately needs structure but cannot maintain it, who is profoundly bored by routine but deeply unsettled by change.
One participant in the study described it this way: “My autism creates a need for order, formality, structure, routines, repetition, solitude, and intense interests, all of which are disrupted by my ADHD’s chaotic impulse towards newness, variety, inconsistency, and inattention.”
Sensory experience becomes particularly fraught. A woman with AuDHD might be highly reactive to certain sounds or textures while simultaneously seeking out intense sensory input like loud music or deep pressure. Her needs can fluctuate minute to minute, leaving her feeling perpetually out of sync with her environment.
The social dimension is equally complex. ADHD often produces impulsivity and a desire for social connection, while autism can make social interaction exhausting and require careful pre-planning. A woman with AuDHD might come across as outgoing and socially motivated, which masks her autistic traits, or she might appear unusually detail-oriented and rule-following, which masks her ADHD.
This mutual masking effect is one reason why women with both conditions are so often missed entirely. As ADDitude Magazine reported, “An AuDHD woman might be too socially motivated to fit classic autism presentations, yet too detail-oriented and rule-following to match typical ADHD presentations.” She falls through every diagnostic crack.
A 2025 analysis of 1.9 million insurance claims found that 45% of adults with ADHD show significant autistic traits, yet only 1.7% carry a co-existing autism diagnosis. The gap suggests that the vast majority of people living with both conditions have been identified with only one, if they’ve been identified at all.
Instead of a unifying diagnosis, these women collect fragments: anxiety here, depression there, an eating disorder in college, chronic fatigue that no one can explain. Each label addresses a symptom without ever identifying the source.
A 2025 study in Scientific Reports found that women who received late ADHD diagnoses reported pervasive feelings of guilt, shame, and low self-esteem that had accumulated over years of struggling without explanation. (Photo source: Canva)
The Comorbidity Spiral
Here is the cruelest part of this story: the missed diagnosis doesn’t just delay treatment. It actively creates new conditions to treat.
Years of undiagnosed ADHD produce chronic stress, and chronic stress rewires the brain and body in measurable ways. The hypothalamic-pituitary-adrenal axis, which regulates the stress response, becomes dysregulated. Inflammation increases. Sleep architecture deteriorates. The conditions associated with “mental health” begin to emerge not as primary disorders but as downstream consequences of a nervous system that has never been allowed to rest.
Depression develops in women who have spent decades believing they are fundamentally flawed, lazy, or stupid. Anxiety takes hold in women who have learned that any moment of relaxation will be punished by a forgotten deadline or missed appointment. Eating disorders emerge as attempts to control something, anything, when the internal world feels so chaotic.
The research on chronic pain is particularly striking. A Swedish longitudinal study published in the Journal of Pain Research followed children diagnosed with ADHD and autism into young adulthood and found that 76.6% of women with these conditions reported chronic pain. The study also found that women with ADHD who were treated with stimulant medication had significantly lower rates of chronic widespread pain, suggesting that addressing the underlying condition may prevent some of the physical consequences.
Then there is rejection sensitive dysphoria, or RSD, a term that describes the intense emotional pain triggered by perceived rejection or criticism. Between 34% and 70% of people with ADHD experience significant emotional dysregulation, and women with ADHD report higher rates of RSD than men. The condition is not recognized in the Diagnostic and Statistical Manual of Mental Disorders and is frequently misdiagnosed as borderline personality disorder, bipolar disorder, or generalized anxiety.
By age 12, research suggests, children with ADHD have received approximately 20,000 more negative or corrective messages than their neurotypical peers. Twenty thousand times they have been told they’re doing it wrong, not paying attention, not trying hard enough. The emotional scar tissue from that accumulation of criticism doesn’t simply disappear with an adult diagnosis.
By the time a woman finally receives the correct diagnosis, she is often treating not just ADHD but the full cascade of conditions that developed in its absence. The original missed diagnosis has metastasized into a complex clinical picture that requires multiple interventions, multiple medications, and years of therapeutic work to untangle.
The Perimenopause Trigger
For many women, the tipping point comes in their 40s. The compensatory mechanisms that held everything together for decades begin to fail, and the symptoms that were always there become impossible to ignore.
The culprit is estrogen. As hormone levels fluctuate and decline during perimenopause, so does the brain’s supply of dopamine and serotonin, the neurotransmitters most directly implicated in ADHD. The woman who managed her symptoms through sheer force of will suddenly finds that will is no longer enough.
A January 2026 study from Monash University found that 97% of women with ADHD reported their symptoms worsened during menopause. The same study found that 88% noticed changes in their ADHD symptoms across their menstrual cycle, and 70% reported symptoms worsening after having a baby. Hormonal transitions, the researchers concluded, are not incidental to ADHD in women. They are central to how the condition is experienced across the lifespan.
Research published in European Psychiatry found that women with ADHD experience perimenopausal symptoms up to 10 years earlier than women without the condition. A survey of more than 4,000 women by ADDitude Magazine found that 70% said ADHD had a “life-altering” impact during their 40s and 50s.
This is when many women receive their first ADHD diagnosis. They arrive at their doctor’s office complaining of brain fog, memory problems, difficulty concentrating, and emotional volatility. These symptoms are often attributed to menopause itself, but for women with underlying ADHD, the hormonal shift has simply stripped away the last of their compensatory reserves.
Sara Kelly, an ADHD coach who was herself diagnosed in midlife, describes the experience on her Instagram: “If you are a woman with ADHD in your forties or fifties, there is a very particular kind of quiet panic that can sneak up on you.” The strategies that worked for decades stop working. The scaffolding collapses. And the question that emerges is the same one millions of women have asked: How did I go my whole life without realizing this was ADHD?
What Recognition Looks Like
The diagnosis, when it finally comes, is rarely simple relief. It is grief and vindication and rage all tangled together.
“Women come to me after decades of being told they’re anxious or depressed,” says Kojo Sarfo, a psychiatric-mental health nurse practitioner. “They’ve been treated for everything except what they actually have.”
The realization that struggle was not inevitable, that there were explanations and treatments and accommodations that could have been available decades earlier, can be destabilizing. Women describe mourning the lives they might have lived, the careers they might have sustained, the relationships they might have kept, if only someone had seen them clearly.
But recognition also opens a door. Late diagnosis means access to medication, coaching, and therapeutic approaches specifically designed for the ADHD brain. It means finally having language for experiences that previously felt like personal failings. It means finding community with other women who understand the particular exhaustion of masking for decades.
“Most autism experts basically end their expertise with diagnosis,” notes Professor Sol Smith, a late-diagnosed educator. “A professional tells you, ‘Yes, you are autistic,’ and you’re just on your own again.” The same is often true for ADHD. Diagnosis is not the end of the journey. It is the beginning of a different one.
For women still seeking answers, the path forward requires both systemic change and individual advocacy. It means pushing for diagnostic criteria that reflect how ADHD actually presents in girls and women. It means training clinicians to look beyond the hyperactive-boy model. It means believing women when they describe their own experiences rather than dismissing their symptoms as anxiety, depression, or simply the overwhelm of modern life.
And for the women who have already spent decades undiagnosed, it means something simpler and harder: learning to extend to themselves the understanding they were never given. They were not broken. They were not lazy or stupid or fundamentally flawed. They were navigating a world that was not built for their brains, without a map, without support, and without even knowing there was a different way to be.
They were undiagnosed. And now, finally, they know.





